


You’ve come to know that your APEX crew likes to examine the history of how we got to where we are. In the case of oral endotracheal intubation (OETI), an essential skill CRNAs perform with aplomb, we find evidence of its origins from Hindu scripts dating over 4000 years ago as a hollow reed surgically inserted into the trachea. A quantum leap forward to just 126 years ago, Bretonneau, who first termed the obstructive membranous disease “diphtheria,” described surgical tracheostomy as a lifesaving therapeutic intervention. Today, we’re taking a look at the laryngoscope, specifically traditional, direct vs video laryngoscopy.
| Table of Contents
- Historical foundations
- Where the typewriter enters the picture
- Traditional direct laryngoscopy vs video laryngoscopy
- Retiring traditional, direct laryngoscopy
- Where we are today
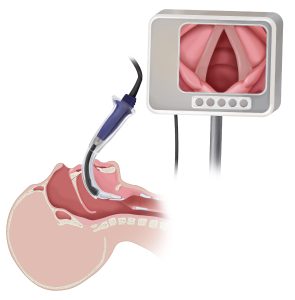
The history of the laryngoscope

Macewen formally described the first OETI during surgical anesthesia in 1880, but it wasn’t until WWI, that Magill advocated for its widespread adoption. Magill, Miller, and Macintosh developed hand-held laryngoscopes still used today. Intubation was often performed under less-than-ideal conditions, with patients often experiencing duress and dental trauma. With curare’s introduction in 1942, we had a dual-purpose drug that relaxed abdominal muscles and facilitated laryngoscopy. OETI was on a roll!
And then, of course, the advent of videolaryngoscopy (VL)

Pacey crafted the Glidescope™ in 1999 using a modified arthroscopic optical instrument, a eureka moment in airway management with other devices to follow. This proved a welcome evolution as practitioners now had various tools to perform OETI. Of interest is that the early publications introducing VL portrayed the technology as “difficult airway devices.”
So, where does the typewriter enter the picture?
The humble typewriter represented a quantum technological leap beyond using pen and paper. The tool’s legibility, durability, and efficiency benefited the literary, business, education, and scientific communities. However, with the emergence of small computers with word-processing and auto-correction capabilities, its precursor, the humble typewriter, seemed more like a dinosaur.
Consider how home streaming vanquished VHS cassettes, digital music players eclipsed eight-track tapes, DVDs retired reel-to-reel movies, and cell phones dispatched the need for fixed-line phones. New technologies displace older ones, it’s as predictable as the sun rising in the east and setting in the west.
Is our traditional laryngoscope experiencing a similar fate? Is it being supplanted by VL in a manner akin to how the computer displaced the typewriter?
What the evidence reveals: Traditional direct laryngoscopy vs video laryngoscopy?

The conclusion is obvious if we look solely at the substantial published literature involving in-hospital, anesthesia-care, and ICU scenarios. VL improves the view, eases laryngoscopy, and increases the first-try success of ETT placement. Furthermore, it achieves this end without increasing adverse events and, in most cases, appears to prevent them. Support comes from individual trials, but more impressively from the robust and strongly weighted findings demonstrated in systematic reviews and metanalyses.

Many studies employed assessments of optical performance and provided mechanical and cognitive demand, demonstrating the superiority of VL. Additionally, VL may find its greatest asset in known or unexpected difficult airway cases. The recent ASA Difficult Airway Algorithm addresses this point. It notes that metanalyses of randomized trials using video vs direct laryngoscopy in anticipated difficult airways resulted in better views, greater success, and fewer maneuvers than direct laryngoscopy.
The most recent single trial we found serves as a case in point. This study, conducted over 3 years, included 26,692 consecutive OETIs in adults having surgery in two matched hospitals. Following a period of education regarding VL in one and no such intervention in the other, VL as a 1st-choice approach rose from 0.27% to 66% in the former. Before the study intervention, the rate of an “easy” airway increased from 94.3% to 98.7%. Providers reporting significant airway challenges decreased from 5.3% to 1.9%, a three-fold decline. Difficult laryngoscopy and the need for airway rescue decreased. No changes in the measured outcomes were seen in the comparison hospital with no intervention.
The study used a Macintosh (curved blade) style VL as the intervention. The authors concluded that VL as the 1st-choice for OETI resulted in a clinically significant increase in the proportion of easy intubations compared with the traditional Macintosh laryngoscope approach.
Case closed: We should retire traditional, direct laryngoscopy
Not so fast! While new technologies drive out older ones, in a manner your APEX crew terms ‘evolutionary obsolescence,’ attendant questions must be addressed. Concerning VL vs traditional direct laryngoscopy, let’s pose just a few:
- Are there differences in how different types of VLs perform?
- Are there scenarios where direct laryngoscopy might be superior?
- What are the economics of VL becoming the standard of care?
- How might universal VL affect entry-level education and training?
- Does VL have a complication profile we’ve yet to appreciate?
- Should VL emphasize single use or reusability of equipment?
So, Where Are We Today?
From our careful reading of the literature, we came away with the following conclusions:
- The evidence favors VL in achieving first-pass OETI.
- The evidence reveals VL reduces failure to intubate and esophageal intubation.
- Video is the go-to in difficult airway scenarios.
- VL is not without complications and is not always successful in achieving tracheal intubation.
- Direct laryngoscopy competency skills may suffer due to disuse if VL predominates.
- The cost of outfitting all anesthetizing and resuscitation platforms will be substantial.
- VL device failure is possible, with direct laryngoscopy the default.
We’ve experienced an influx of new technologies in our anesthesia practice. Examples include electronic medical records, “smart” patient monitors, increasingly sophisticated anesthesia workstations, ICU-caliber ventilators, ultrasound tools, and a depth of anesthesia devices. To the mix, we now have many different VL technologies.
No amount of pro-VL research will likely extinguish our access to, or skill with, direct laryngoscopy, a technique that exemplifies the CRNA as an airway expert. That said, there is agreement that taking all the necessary steps to optimize the 1st-attempt success is essential.
Few undertake a major writing project using the typewriter instead of a word-processing app on a computer. Likewise, most are likely to favor using videolaryngoscopy when encountering a known difficult airway. Since the evidence is clear that unanticipated difficult airways still occur routinely, there is logic that if VL is not first up-to-bat in all cases, it should be immediately available.
Related Articles



