


We’ve recently become aware of pediatric cases, one currently under litigation, where the outcome in the dental office went very poorly. We want to examine the issue central to these cases, pertaining to local anesthetic toxicity, which demands our clinical consideration and the imperative to share our knowledge with others. The use of local anesthesia (LA) in the dentist’s office is not without its peril.
We generally think of LAST (local anesthetic systemic toxicity) as a complication occurring during peripheral nerve blocks, where an inadvertent intravascular injection of LA creates CNS and/or cardiovascular chaos. A very poor outcome may result if the event is not rapidly recognized, followed by swift and effective treatment.
Table of Contents
- A Scan of Pediatric Dental Literature on Local Anesthetic Hazards
- The American Academy of Pediatric Dentistry (AAPD) Weighs in on the Best Practices of Local Anesthetic Use in Children
- Lipid Rescue Therapy for LAST in Pediatric Dentistry
- What Can We Take Away About Local Anesthetic Toxicity in Pediatric Dentistry?
Anesthesia hazards in pediatric dentistry according to literature
A recent article in Dental Clinics of North America, titled “Updates of topical local anesthesia agents” carefully notes that those who provide care to toddlers and children must be aware of the particularly “low safety margin” (emphasis by the authors) of local anesthetics. They cite literature demonstrating significant hypotension, respiratory depression, and cardiac arrest that may result. The authors reference the “number of local anesthetic-induced toxicities involving children” as deeply concerning.
A review of the different injectable and topical local anesthetics is provided with commentary. We were dismayed to see no mention of methemoglobinemia regarding the topical applications of benzocaine and lidocaine. CRNAs are aware of the danger of methemoglobinemia with these drugs, where the ferrous (Fe2+) form of iron is oxidized to the ferric (Fe3+) state, rendering it unable to bind O2, resulting in tissue hypoxia and, if untreated, possibly death.
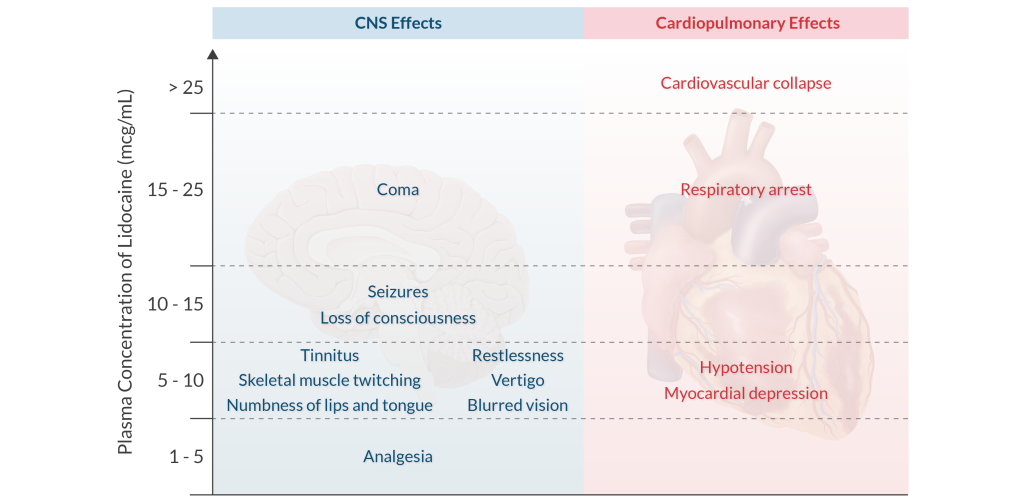
We were also concerned about not seeing the prodromes of systemic toxicity, such as circumoral numbness, tinnitus, blurred vision, or metallic taste mentioned. The word “seizure” is only found once, buried in an accompanying table that may be missed entirely without an exacting read. CRNAs know that local anesthetic toxicity evolves progressively, and once CNS symptoms occur, the patient is on the precipice of experiencing what may be catastrophic cardiovascular toxicity.
The only mention of bupivacaine in the paper is as follows:
“It is not recommended for pediatrics or physically/mentally disabled patients because of prolonged effects, which increase the risk of soft tissue injury.” There is no mention of bupivacaine’s extraordinary potential to cause catastrophic myocardial toxicity.
The American Academy of Pediatric Dentistry’s (AAPD) view on local anesthetic use in children
We found a freshly published 2023 white paper prompted by concerns about pediatric dentists’ inconsistent appreciation for local anesthetic toxicity. This collaborative effort by the AAPD’s Council on Clinical and Scientific Affairs is intended to inform and recommend best practices regarding using local anesthetics in infants, children, and adolescents during dental procedures. The AAPD notes that the document primarily intends to help pediatric dentists make informed decisions when using local anesthetics in their patient populations.

While we applauded the authors of the AAPD document for detailing the risk of methemoglobinemia with the use of benzocaine, prilocaine, and lidocaine, we were left with a number of concerns. While they mention that the FDA warns against the use of benzocaine in those < 2 years of age, we were disheartened to find no mention of the treatment of methemoglobinemia.
Similarly, we felt more concern should be raised about using “compounded products.” These custom-made pharmaceuticals prepared in dental offices or local vendors bypass the FDA approval process. Local anesthetics combined with other drugs have unclear potential toxicities.
Local anesthetics and cardiac toxicity
We were also troubled that the document reads, “The cardio-depressant effects of local anesthetics are not seen until there is a significantly elevated level in the blood.” This may lead to a false sense of security and is not in keeping with what we know to be a thin margin between CNS and cardiac toxicity.
Risk of local anesthetic systemic toxicity
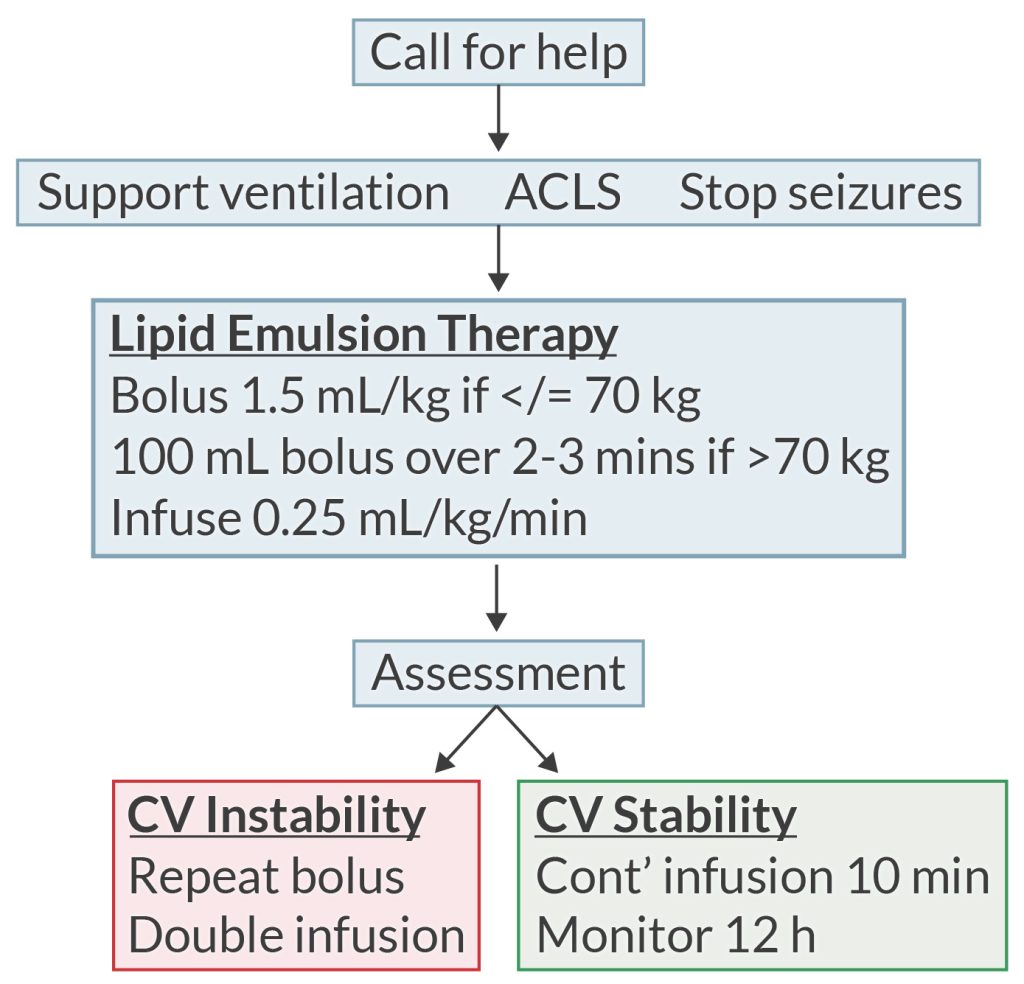
It was gratifying to see a specific section explaining the risk of local anesthetic systemic toxicity (LAST), noting that pediatric patients are at particular risk. Early signs of toxicity are described, with the risk of progression to seizures noted. However, we worry that the only information provided about treating LAST described discontinuing the use of the local anesthetic agent, performing “patient rescue” (rather vague!!), and activating emergency services (calling 911) based on the severity of the reaction.
We were perplexed that while lipid emulsion therapy is “a priority in potentially serious cases,” no dosing or guidance is provided. ACLS guidelines are not provided, nor is their recommended modification, such as avoiding high-dose epinephrine, vasopressin, calcium channel blockers, lidocaine, etc.
We found some very useful suggestions in the document that have a bearing on dental anesthesia practices. The authors correctly reinforced that the risk of toxicity manifests as altered sensorium, muscle twitching, seizures, arrhythmias, and hypotension, noting also that death can occur. We found it useful to remind all of us about the difficulty and unreliability of aspirating before injecting using dental needle gauges in the 23-30 range. There was also mention that the young child’s mandibular bone is less dense than the adult’s, allowing more rapid and complete diffusion of an injected drug systemically.
Our research found an interesting study questioning 124 community dentists’ knowledge and appreciation for local anesthetic toxicity. The results revealed very limited knowledge in the area. The authors concluded that there was a definitive need to improve the knowledge of providers regarding local anesthetic drugs, how they are used, what complications and challenges might arise, and how to manage them.
Lipid rescue therapy for LAST in pediatric dentistry
For our CRNA readers’ review, here are the most recent guidelines regarding lipid rescue embraced by the anesthesiology community.
While any local anesthetic agent may cause systemic toxicity, bupivacaine is most worrisome due to what we term it being a ‘triple-threat.’
- Depresses cardiac conduction and contractility
- Inhibits Na+ and Ca+2 channels
- Slowly dissociates from these channels.
What can we take away about local anesthetic toxicity in pediatric dentistry?
First, be aware of local toxicities. The pediatric dental community needs to be more mindful of the spectrum and risk of local anesthetic toxicities. In training programs and the pediatric dental literature, there should be greater emphasis on the risks of methemoglobinemia and LAST, emphasizing how quickly complications can progress and snowball, and clear guidelines for treating systemic toxicity in the most evidence-based manner.
CRNAs appreciate that being aware of the risk for local anesthetic complications and making every effort to prevent them is critical to the patient’s safety. We know that the early recognition of the signs of a developing adverse event is critical. Furthermore, it is incumbent that the provider administering the drug be educated, trained, and able to rescue the patient using the appropriate resources.
Secondly, we must be educated about anesthesia toxicity. CRNAs are experts in the realm of anesthesia patient safety. Some of us provide services in dental offices and can directly promote patient safety in their interactions with staff and patients. That said, all of us should feel empowered to educate and disseminate information that advances patient safety whenever possible. This might include:
- Talking to your own dental health providers about local anesthetic toxicity.
- Speaking to personnel in your workplace so that they feel empowered to ask questions of their dental providers.
- Conversation with family nurse practitioners, pediatricians, and general family practitioners when possible. Such discussions can seed downstream educational interactions with their clients and patients.
- Chat it up with your anesthesia colleagues—reviewing issues with potentially serious consequences is never redundant.
Your APEX crew firmly believes in the N-of-1 approach to patient safety. That is, no amount of effort is too significant if we can spare just one child from a complication that may prove catastrophic.
As CRNAs ourselves, we understand the challenge of fitting CRNA continuing education credits into your busy schedule. When you’re ready, we’re here to help.
Related Articles



